Pericarditis
P E R I C A R D I T I S
TODAY'S PEARLS
1. Pericarditis: classic EKG findings, diagnostic criteria & framework
2. STEMI criteria on EKG
3. Treatment of pericarditis & ICAP trial
Dr. Ryan presented a patient with a recent URI, admitted with acute-onset, left-sided, pleuritic, chest pain found to have acute pericarditis.
EKG changes in pericarditis
Diffuse ST elevations & PR depressions
Reciprocal PR elevations/ST depressions in V1 & aVr

Pericarditis - Diagnostic Criteria: 2 of 4 needed for diagnosis
1. Sharp, pleuritic chest pain
2. Pericardial friction rub
2. Pericardial friction rub
3. Changes on EKG
4. New or worsening pericardial effusion
~ Dr. Ryan's patient had 3/4 criteria ~
Dr. Ryan's patient experienced an antecedent viral URI which was likely the cause of her pericarditis.
CAUSES OF PERICARDITIS - FRAMEWORK

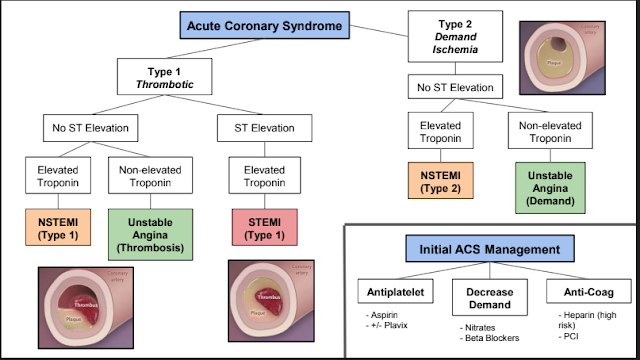
Why isn't this a STEMI? A brief review.
A STEMI will have ST elevations in a single coronary distribution (instead of diffusely) with reciprocal ST depressions & pathologic Q waves( > 1mm x 2mm in lead V1-3). A STEMI will not have PR depressions.
STEMI EKG Criteria (Fourth Universal Definition of MI 2018): ST elevation > 1mm in 2 contiguous leads except V2 or V3 (V2 or V3 need elevations > 1.5mm in women & 2mm in med > 40 years)
TREATMENT OF PERICARDITIS:
Aspirin/NSAIDS +/- Colchicine (no steroids, if you can help it)
ICAP: Imazio M, et al. "A Randomized Trial of Colchicine for Acute Pericarditis". The New England Journal of Medicine. 2013. 369(16):1522-1528.
Randomized patients to colchicine vs. placebo. Patients also received ASA, NSAIDS or prednisone (ASA 71.7%, ibuprofen 20.0%, prednisone 8.3%). Recurrent pericarditis was seen in 16.7% of patients treated with colchicine & 37.5% of patients in the placebo group.

The information posted above is for educational use only by the trainees of a non-profit hospital residency program.
Compiled by: Emma

Comments
Post a Comment